Pes Planus Causes And Treatment
Overview
Pes planus can be part of normal development. Infants typically have a minimal arch. Many toddlers have flattening of the long arch, with forefoot pronation and heel valgus on weight-bearing. There may be ligamentous laxity, which is probably determined genetically. Most of these children spontaneously develop a strong normal arch by around age 10.
Causes
There are several reasons why arches fall. It can be genetic, it can be a result of unsupported shoes, a product of our lives and the pressure we put on the feet. Some people have active lifestyles so the wear and tear effect on the muscles there that runs down the back of the calf and wraps around the arch can slacken as we get older. It can be a number of things.
Symptoms
Pain and stiffness of the medial arch or anywhere along the mid-portion of the foot. Associated discomfort within and near the ankle joint. The knees, hips, and lower back may be the primary source of discomfort. Feet may often feel tired and achy. Painful shin splints may develop with activity. Gait may be awkward.
Diagnosis
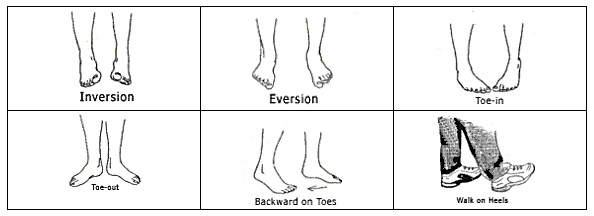
If your child has flatfeet, his or her doctor will ask about any family history of flatfeet or inherited foot problems. In a person of any age, the doctor will ask about occupational and recreational activities, previous foot trauma or foot surgery and the type of shoes worn. The doctor will examine your shoes to check for signs of excessive wear. Worn shoes often provide valuable clues to gait problems and poor bone alignment. The doctor will ask you to walk barefoot to evaluate the arches of the feet, to check for out-toeing and to look for other signs of poor foot mechanics. The doctor will examine your feet for foot flexibility and range of motion and feel for any tenderness or bony abnormalities. Depending on the results of this physical examination, foot X-rays may be recommended. X-rays are always performed in a young child with rigid flatfeet and in an adult with acquired flatfeet due to trauma.
how to fix fallen arches
Non Surgical Treatment
Heel cord stretching is an important part of treatment, as a tight Achilles tendon tends to pronate the foot. Orthotics (inserts or insoles, often custom-made) may be used. These usually contain a heel wedge to correct calcaneovalgus deformity, and an arch support. This is the usual treatment for flexible Pes Planus (if treatment is needed). A suitable insole can help to correct the deformity while it is worn. Possibly it may prevent progression of flat feet, or may reduce symptoms. However, the effectiveness of arch support insoles is uncertain. Arch supports used without correcting heel cord contracture can make symptoms worse. In patients with fixed Pes planus or arthropathy, customised insoles may relieve symptoms. Reduce contributing factors, wear shoes with low heels and wide toes. Lose weight if appropriate. Do exercises to strengthen foot muscles - walking barefoot (if appropriate), toe curls (flexing toes) and heel raises (standing on tiptoe).
Surgical Treatment

This is rare and usually only offered if patients have significant abnormalities in their bones or muscles. Treatments include joint fusion, reshaping the bones in the foot, and occasionally moving around tendons in the foot to help balance out the stresses (called tendon transfer). Flat feet and fallen arches are common conditions that are in most cases asymptomatic. However, in patients who do have symptoms, treatments are available that can help reduce pain and promote efficient movement. Orthotic devices are well recognised as an excellent treatment and podiatrists can offer these different treatment modalities as individualised treatments for patients.
Prevention
It?s time to take a long hard look at what?s in your closet. Now is the time to toss out shoes that are well worn. You also need to say good-bye to thin-soled shoes that offer zero arch support. If you?re overweight, fallen arches may be a sign the universe is trying to tell you something. You need to lose weight, and odds are, fallen arches are but one of many physical discomforts you are experiencing.
After Care
Patients may go home the day of surgery or they may require an overnight hospital stay. The leg will be placed in a splint or cast and should be kept elevated for the first two weeks. At that point, sutures are removed. A new cast or a removable boot is then placed. It is important that patients do not put any weight on the corrected foot for six to eight weeks following the operation. Patients may begin bearing weight at eight weeks and usually progress to full weightbearing by 10 to 12 weeks. For some patients, weightbearing requires additional time. After 12 weeks, patients commonly can transition to wearing a shoe. Inserts and ankle braces are often used. Physical therapy may be recommended. There are complications that relate to surgery in general. These include the risks associated with anesthesia, infection, damage to nerves and blood vessels, and bleeding or blood clots. Complications following flatfoot surgery may include wound breakdown or nonunion (incomplete healing of the bones). These complications often can be prevented with proper wound care and rehabilitation. Occasionally, patients may notice some discomfort due to prominent hardware. Removal of hardware can be done at a later time if this is an issue. The overall complication rates for flatfoot surgery are low.
Pes planus can be part of normal development. Infants typically have a minimal arch. Many toddlers have flattening of the long arch, with forefoot pronation and heel valgus on weight-bearing. There may be ligamentous laxity, which is probably determined genetically. Most of these children spontaneously develop a strong normal arch by around age 10.
Causes
There are several reasons why arches fall. It can be genetic, it can be a result of unsupported shoes, a product of our lives and the pressure we put on the feet. Some people have active lifestyles so the wear and tear effect on the muscles there that runs down the back of the calf and wraps around the arch can slacken as we get older. It can be a number of things.
Symptoms
Pain and stiffness of the medial arch or anywhere along the mid-portion of the foot. Associated discomfort within and near the ankle joint. The knees, hips, and lower back may be the primary source of discomfort. Feet may often feel tired and achy. Painful shin splints may develop with activity. Gait may be awkward.
Diagnosis
If your child has flatfeet, his or her doctor will ask about any family history of flatfeet or inherited foot problems. In a person of any age, the doctor will ask about occupational and recreational activities, previous foot trauma or foot surgery and the type of shoes worn. The doctor will examine your shoes to check for signs of excessive wear. Worn shoes often provide valuable clues to gait problems and poor bone alignment. The doctor will ask you to walk barefoot to evaluate the arches of the feet, to check for out-toeing and to look for other signs of poor foot mechanics. The doctor will examine your feet for foot flexibility and range of motion and feel for any tenderness or bony abnormalities. Depending on the results of this physical examination, foot X-rays may be recommended. X-rays are always performed in a young child with rigid flatfeet and in an adult with acquired flatfeet due to trauma.
how to fix fallen arches
Non Surgical Treatment
Heel cord stretching is an important part of treatment, as a tight Achilles tendon tends to pronate the foot. Orthotics (inserts or insoles, often custom-made) may be used. These usually contain a heel wedge to correct calcaneovalgus deformity, and an arch support. This is the usual treatment for flexible Pes Planus (if treatment is needed). A suitable insole can help to correct the deformity while it is worn. Possibly it may prevent progression of flat feet, or may reduce symptoms. However, the effectiveness of arch support insoles is uncertain. Arch supports used without correcting heel cord contracture can make symptoms worse. In patients with fixed Pes planus or arthropathy, customised insoles may relieve symptoms. Reduce contributing factors, wear shoes with low heels and wide toes. Lose weight if appropriate. Do exercises to strengthen foot muscles - walking barefoot (if appropriate), toe curls (flexing toes) and heel raises (standing on tiptoe).
Surgical Treatment
This is rare and usually only offered if patients have significant abnormalities in their bones or muscles. Treatments include joint fusion, reshaping the bones in the foot, and occasionally moving around tendons in the foot to help balance out the stresses (called tendon transfer). Flat feet and fallen arches are common conditions that are in most cases asymptomatic. However, in patients who do have symptoms, treatments are available that can help reduce pain and promote efficient movement. Orthotic devices are well recognised as an excellent treatment and podiatrists can offer these different treatment modalities as individualised treatments for patients.
Prevention
It?s time to take a long hard look at what?s in your closet. Now is the time to toss out shoes that are well worn. You also need to say good-bye to thin-soled shoes that offer zero arch support. If you?re overweight, fallen arches may be a sign the universe is trying to tell you something. You need to lose weight, and odds are, fallen arches are but one of many physical discomforts you are experiencing.
After Care
Patients may go home the day of surgery or they may require an overnight hospital stay. The leg will be placed in a splint or cast and should be kept elevated for the first two weeks. At that point, sutures are removed. A new cast or a removable boot is then placed. It is important that patients do not put any weight on the corrected foot for six to eight weeks following the operation. Patients may begin bearing weight at eight weeks and usually progress to full weightbearing by 10 to 12 weeks. For some patients, weightbearing requires additional time. After 12 weeks, patients commonly can transition to wearing a shoe. Inserts and ankle braces are often used. Physical therapy may be recommended. There are complications that relate to surgery in general. These include the risks associated with anesthesia, infection, damage to nerves and blood vessels, and bleeding or blood clots. Complications following flatfoot surgery may include wound breakdown or nonunion (incomplete healing of the bones). These complications often can be prevented with proper wound care and rehabilitation. Occasionally, patients may notice some discomfort due to prominent hardware. Removal of hardware can be done at a later time if this is an issue. The overall complication rates for flatfoot surgery are low.
Leg Length Discrepancy Symptoms
Overview
Large leg length inequalities can be treated by staged lengthenings or by simultaneous ipsilateral femoral and tibial lengthenings. Additionally, lengthenings can be combined with appropriately timed epiphysiodesis in an effort to produce leg length equality. Staged lengthenings are often used for congenital deficiencies such as fibular hemimelia, in which 15 cm or more may be needed to produce leg length equality. We typically plan for the final lengthening to be completed by age 13 or 14 years, and allow at least 3 years between lengthenings. Lengthening of both the tibia and femur simultaneously requires aggressive therapy and treatment of soft tissue contractures. Curran et al[57] reported the need for surgical release of soft tissue contractures in 3 of 8 patients treated with simultaneous ipsilateral femoral and tibial lengthenings. Lengthening over an IM nail can be done in an effort to decrease the amount of time the fixator needs to be worn and to prevent angular malalignment. This technique requires that the patient be skeletally mature and it carries a higher risk of osteomyelitis (up to 15%). Additionally, if premature consolidation occurs, a repeat corticotomy is more difficult.
Causes
From an anatomical stand point, the LLD could have been from hereditary, broken bones, diseases and joint replacements. Functional LLD can be from over pronating, knee deformities, tight calves and hamstrings, weak IT band, curvature in the spine and many other such muscular/skeletal issues.
Symptoms
In addition to the distinctive walk of a person with leg length discrepancy, over time, other deformities may be noted, which help compensate for the condition. Toe walking on the short side to decrease the swaying during gait. The foot will supinate (high arch) on the shorter side. The foot will pronate (flattening of the arch) on the longer side. Excessive pronation leads to hypermobility and instability, resulting in metatarsus primus varus and associated unilateral juvenile hallux valgus (bunion) deformity.
Diagnosis
The only way to decipher between anatomical and functional leg length inequalities (you can have both) is by a physical measurement and series of biomechanical tests. It is actually a simple process and gets to the true cause of some runner?s chronic foot, knee, hip and back pain. After the muscles are tested and the legs are measured it may be necessary to get a special X-ray that measures both of your thighs (Femurs) and legs (Tibias). The X-ray is read by a medical radiologist who provides a report of the actual difference down to the micrometer leaving zero room for error. Once the difference in leg length is known, the solution becomes clear.
Non Surgical Treatment
The non-surgical intervention is mainly usedfor the functional and environmental types of leg length discrepancies. It is also applied to the mild category of limb length inequality. Non-surgical intervention consists of stretching the muscles of the lower extremity. This is individually different, whereby the M. Tensor Fascia latae, the adductors, the hamstring muscles, M. piriformis and M. Iliopsoas are stretched. In this non-surgical intervention belongs also the use of shoe lifts. These shoe lifts consists of either a shoe insert (up to 10-20mm of correction), or building up the sole of the shoe on the shorter leg (up to 30-60mm of correction). This lift therapy should be implemented gradually in small increments. Several studies have examined the treatment of low back pain patients with LLD with shoe lifts. Gofton obtained good results: the patients experienced major or complete pain relief that lasted upon follow-up ranging from 3 to 11 years. Helliwell also observed patients whereby 44% experienced complete pain relief, and 45% had moderate or substantial pain relief. Friberg found that 157 (of 211) patients with LBP, treated with shoe lifts, were symprom-free after a mean follow-up of 18 months.

shoe lifts for uneven legs
Surgical Treatment
Large leg length inequalities can be treated by staged lengthenings or by simultaneous ipsilateral femoral and tibial lengthenings. Additionally, lengthenings can be combined with appropriately timed epiphysiodesis in an effort to produce leg length equality. Staged lengthenings are often used for congenital deficiencies such as fibular hemimelia, in which 15 cm or more may be needed to produce leg length equality. We typically plan for the final lengthening to be completed by age 13 or 14 years, and allow at least 3 years between lengthenings. Lengthening of both the tibia and femur simultaneously requires aggressive therapy and treatment of soft tissue contractures. Curran et al[57] reported the need for surgical release of soft tissue contractures in 3 of 8 patients treated with simultaneous ipsilateral femoral and tibial lengthenings. Lengthening over an IM nail can be done in an effort to decrease the amount of time the fixator needs to be worn and to prevent angular malalignment. This technique requires that the patient be skeletally mature and it carries a higher risk of osteomyelitis (up to 15%). Additionally, if premature consolidation occurs, a repeat corticotomy is more difficult.
Large leg length inequalities can be treated by staged lengthenings or by simultaneous ipsilateral femoral and tibial lengthenings. Additionally, lengthenings can be combined with appropriately timed epiphysiodesis in an effort to produce leg length equality. Staged lengthenings are often used for congenital deficiencies such as fibular hemimelia, in which 15 cm or more may be needed to produce leg length equality. We typically plan for the final lengthening to be completed by age 13 or 14 years, and allow at least 3 years between lengthenings. Lengthening of both the tibia and femur simultaneously requires aggressive therapy and treatment of soft tissue contractures. Curran et al[57] reported the need for surgical release of soft tissue contractures in 3 of 8 patients treated with simultaneous ipsilateral femoral and tibial lengthenings. Lengthening over an IM nail can be done in an effort to decrease the amount of time the fixator needs to be worn and to prevent angular malalignment. This technique requires that the patient be skeletally mature and it carries a higher risk of osteomyelitis (up to 15%). Additionally, if premature consolidation occurs, a repeat corticotomy is more difficult.
Causes
From an anatomical stand point, the LLD could have been from hereditary, broken bones, diseases and joint replacements. Functional LLD can be from over pronating, knee deformities, tight calves and hamstrings, weak IT band, curvature in the spine and many other such muscular/skeletal issues.
Symptoms
In addition to the distinctive walk of a person with leg length discrepancy, over time, other deformities may be noted, which help compensate for the condition. Toe walking on the short side to decrease the swaying during gait. The foot will supinate (high arch) on the shorter side. The foot will pronate (flattening of the arch) on the longer side. Excessive pronation leads to hypermobility and instability, resulting in metatarsus primus varus and associated unilateral juvenile hallux valgus (bunion) deformity.
Diagnosis
The only way to decipher between anatomical and functional leg length inequalities (you can have both) is by a physical measurement and series of biomechanical tests. It is actually a simple process and gets to the true cause of some runner?s chronic foot, knee, hip and back pain. After the muscles are tested and the legs are measured it may be necessary to get a special X-ray that measures both of your thighs (Femurs) and legs (Tibias). The X-ray is read by a medical radiologist who provides a report of the actual difference down to the micrometer leaving zero room for error. Once the difference in leg length is known, the solution becomes clear.
Non Surgical Treatment
The non-surgical intervention is mainly usedfor the functional and environmental types of leg length discrepancies. It is also applied to the mild category of limb length inequality. Non-surgical intervention consists of stretching the muscles of the lower extremity. This is individually different, whereby the M. Tensor Fascia latae, the adductors, the hamstring muscles, M. piriformis and M. Iliopsoas are stretched. In this non-surgical intervention belongs also the use of shoe lifts. These shoe lifts consists of either a shoe insert (up to 10-20mm of correction), or building up the sole of the shoe on the shorter leg (up to 30-60mm of correction). This lift therapy should be implemented gradually in small increments. Several studies have examined the treatment of low back pain patients with LLD with shoe lifts. Gofton obtained good results: the patients experienced major or complete pain relief that lasted upon follow-up ranging from 3 to 11 years. Helliwell also observed patients whereby 44% experienced complete pain relief, and 45% had moderate or substantial pain relief. Friberg found that 157 (of 211) patients with LBP, treated with shoe lifts, were symprom-free after a mean follow-up of 18 months.
shoe lifts for uneven legs
Surgical Treatment
Large leg length inequalities can be treated by staged lengthenings or by simultaneous ipsilateral femoral and tibial lengthenings. Additionally, lengthenings can be combined with appropriately timed epiphysiodesis in an effort to produce leg length equality. Staged lengthenings are often used for congenital deficiencies such as fibular hemimelia, in which 15 cm or more may be needed to produce leg length equality. We typically plan for the final lengthening to be completed by age 13 or 14 years, and allow at least 3 years between lengthenings. Lengthening of both the tibia and femur simultaneously requires aggressive therapy and treatment of soft tissue contractures. Curran et al[57] reported the need for surgical release of soft tissue contractures in 3 of 8 patients treated with simultaneous ipsilateral femoral and tibial lengthenings. Lengthening over an IM nail can be done in an effort to decrease the amount of time the fixator needs to be worn and to prevent angular malalignment. This technique requires that the patient be skeletally mature and it carries a higher risk of osteomyelitis (up to 15%). Additionally, if premature consolidation occurs, a repeat corticotomy is more difficult.
All You Need To Understand About Heel Painfulness
Overview

The most common form of heel pain, is pain on the bottom of the heel. It tends to occur for no apparent reason and is often worse when first placing weight on the foot. Patients often complain of pain the first thing in the morning or after getting up to stand after sitting. The pain can be a sharp, searing pain or present as a tearing feeling in the bottom of the heel. As the condition progresses there may be a throbbing pain after getting off your feet or there may be soreness that radiates up the back of the leg. Pain may also radiate into the arch of the foot.
Causes
Heel pain can have many causes but the vast majority is caused by plantar fasciitis. Plantar means, ?bottom of the foot.? Fascia is a ligament or ?bundle? of ligaments. The plantar fascia is the thick ligament that helps to hold up the foot and provide spring in our step. Plantar fasciitis is an inflammation of the plantar fascia and causes more than 90% of heel pain among adults in the US. Plantar fasciitis can be acute, that is, as simple strain of the ligament but often is chronic, hanging on for months if not years. Why does that happen? The answer is poor foot mechanics, the foot sinking down too far allowing the plantar fascia to overstretch with each step taken.
Symptoms
The heel can be painful in many different ways, depending on the cause. Plantar fasciitis commonly causes intense heel pain along the bottom of the foot during the first few steps after getting out of bed in the morning. This heel pain often goes away once you start to walk around, but it may return in the late afternoon or evening. Although X-ray evidence suggests that about 10% of the general population has heels spurs, many of these people do not have any symptoms. In others, heel spurs cause pain and tenderness on the undersurface of the heel that worsen over several months. In a child, this condition causes pain and tenderness at the lower back portion of the heel. The affected heel is often sore to the touch but not obviously swollen. Bursitis involving the heel causes pain in the middle of the undersurface of the heel that worsens with prolonged standing and pain at the back of the heel that worsens if you bend your foot up or down. Pump bump, this condition causes a painful enlargement at the back of the heel, especially when wearing shoes that press against the back of the heel. Heel bruises, like bruises elsewhere in the body, may cause pain, mild swelling, soreness and a black-and-blue discoloration of the skin. Achilles tendonitis, this condition causes pain at the back of the heel where the Achilles tendon attaches to the heel. The pain typically becomes worse if you exercise or play sports, and it often is followed by soreness, stiffness and mild swelling. A trapped nerve can cause pain, numbness or tingling almost anywhere at the back, inside or undersurface of the heel. In addition, there are often other symptoms, such as swelling or discoloration - if the trapped nerve was caused by a sprain, fracture or other injury.
Diagnosis
The diagnosis of heel pain and heel spurs is made by a through history of the course of the condition and by physical exam. Weight bearing x-rays are useful in determining if a heel spur is present and to rule out rare causes of heel pain such as a stress fracture of the heel bone, the presence of bone tumors or evidence of soft tissue damage caused by certain connective tissue disorders.
Non Surgical Treatment
There are a number of treatments that can help relieve heel pain and speed up your recovery. These include resting your heel, try to avoid walking long distances and standing for long periods, regular stretching, stretching your calf muscles and plantar fascia, pain relief, using an icepack on the affected heel and taking painkillers, such as non-steroidal anti-inflammatory drugs (NSAIDs), wearing good-fitting shoes that support and cushion your foot, running shoes are particularly useful, using supportive devices such as orthoses (rigid supports that are put inside the shoe) or strapping. Around four out of five cases of heel pain resolve within a year. However, having heel pain for this length of time can often be frustrating and painful. In around one in 20 cases, the above treatments are not enough, and surgery may be recommended to release the plantar fascia.
Surgical Treatment
Surgery is a last resort in the treatment of heel pain. Physicians have developed many procedures in the last 100 years to try to cure heel pain. Most procedures that are commonly used today focus on several areas, remove the bone spur (if one is present), release the plantar fascia (plantar fasciotomy), release pressure on the small nerves in the area. Usually the procedure is done through a small incision on the inside edge of the foot, although some surgeons now perform this type of surgery using an endoscope. An endoscope is a tiny TV camera that can be inserted into a joint or under the skin to allow the surgeon to see the structures involved in the surgery. By using the endoscope, a surgeon can complete the surgery with a smaller incision and presumably less damage to normal tissues. It is unclear whether an endoscopic procedure for this condition is better than the traditional small incision. Surgery usually involves identifying the area where the plantar fascia attaches to the heel and releasing the fascia partially from the bone. If a small spur is present this is removed. The small nerves that travel under the plantar fascia are identified and released from anything that seems to be causing pressure on the nerves. This surgery can usually be done on an outpatient basis. This means you can leave the hospital the same day.
heel cushions
Prevention

You can reduce the risk of heel pain in many ways, including. Wear shoes that fit you properly with a firm fastening, such as laces. Choose shoes with shock-absorbent soles and supportive heels. Repair or throw out any shoes that have worn heels. Always warm up and cool down when exercising or playing sport, include plenty of slow, sustained stretches. If necessary, your podiatrist will show you how to tape or strap your feet to help support the muscles and ligaments. Shoe inserts (orthoses) professionally fitted by your podiatrist can help support your feet in the long term.
The most common form of heel pain, is pain on the bottom of the heel. It tends to occur for no apparent reason and is often worse when first placing weight on the foot. Patients often complain of pain the first thing in the morning or after getting up to stand after sitting. The pain can be a sharp, searing pain or present as a tearing feeling in the bottom of the heel. As the condition progresses there may be a throbbing pain after getting off your feet or there may be soreness that radiates up the back of the leg. Pain may also radiate into the arch of the foot.
Causes
Heel pain can have many causes but the vast majority is caused by plantar fasciitis. Plantar means, ?bottom of the foot.? Fascia is a ligament or ?bundle? of ligaments. The plantar fascia is the thick ligament that helps to hold up the foot and provide spring in our step. Plantar fasciitis is an inflammation of the plantar fascia and causes more than 90% of heel pain among adults in the US. Plantar fasciitis can be acute, that is, as simple strain of the ligament but often is chronic, hanging on for months if not years. Why does that happen? The answer is poor foot mechanics, the foot sinking down too far allowing the plantar fascia to overstretch with each step taken.
Symptoms
The heel can be painful in many different ways, depending on the cause. Plantar fasciitis commonly causes intense heel pain along the bottom of the foot during the first few steps after getting out of bed in the morning. This heel pain often goes away once you start to walk around, but it may return in the late afternoon or evening. Although X-ray evidence suggests that about 10% of the general population has heels spurs, many of these people do not have any symptoms. In others, heel spurs cause pain and tenderness on the undersurface of the heel that worsen over several months. In a child, this condition causes pain and tenderness at the lower back portion of the heel. The affected heel is often sore to the touch but not obviously swollen. Bursitis involving the heel causes pain in the middle of the undersurface of the heel that worsens with prolonged standing and pain at the back of the heel that worsens if you bend your foot up or down. Pump bump, this condition causes a painful enlargement at the back of the heel, especially when wearing shoes that press against the back of the heel. Heel bruises, like bruises elsewhere in the body, may cause pain, mild swelling, soreness and a black-and-blue discoloration of the skin. Achilles tendonitis, this condition causes pain at the back of the heel where the Achilles tendon attaches to the heel. The pain typically becomes worse if you exercise or play sports, and it often is followed by soreness, stiffness and mild swelling. A trapped nerve can cause pain, numbness or tingling almost anywhere at the back, inside or undersurface of the heel. In addition, there are often other symptoms, such as swelling or discoloration - if the trapped nerve was caused by a sprain, fracture or other injury.
Diagnosis
The diagnosis of heel pain and heel spurs is made by a through history of the course of the condition and by physical exam. Weight bearing x-rays are useful in determining if a heel spur is present and to rule out rare causes of heel pain such as a stress fracture of the heel bone, the presence of bone tumors or evidence of soft tissue damage caused by certain connective tissue disorders.
Non Surgical Treatment
There are a number of treatments that can help relieve heel pain and speed up your recovery. These include resting your heel, try to avoid walking long distances and standing for long periods, regular stretching, stretching your calf muscles and plantar fascia, pain relief, using an icepack on the affected heel and taking painkillers, such as non-steroidal anti-inflammatory drugs (NSAIDs), wearing good-fitting shoes that support and cushion your foot, running shoes are particularly useful, using supportive devices such as orthoses (rigid supports that are put inside the shoe) or strapping. Around four out of five cases of heel pain resolve within a year. However, having heel pain for this length of time can often be frustrating and painful. In around one in 20 cases, the above treatments are not enough, and surgery may be recommended to release the plantar fascia.
Surgical Treatment
Surgery is a last resort in the treatment of heel pain. Physicians have developed many procedures in the last 100 years to try to cure heel pain. Most procedures that are commonly used today focus on several areas, remove the bone spur (if one is present), release the plantar fascia (plantar fasciotomy), release pressure on the small nerves in the area. Usually the procedure is done through a small incision on the inside edge of the foot, although some surgeons now perform this type of surgery using an endoscope. An endoscope is a tiny TV camera that can be inserted into a joint or under the skin to allow the surgeon to see the structures involved in the surgery. By using the endoscope, a surgeon can complete the surgery with a smaller incision and presumably less damage to normal tissues. It is unclear whether an endoscopic procedure for this condition is better than the traditional small incision. Surgery usually involves identifying the area where the plantar fascia attaches to the heel and releasing the fascia partially from the bone. If a small spur is present this is removed. The small nerves that travel under the plantar fascia are identified and released from anything that seems to be causing pressure on the nerves. This surgery can usually be done on an outpatient basis. This means you can leave the hospital the same day.
heel cushions
Prevention
You can reduce the risk of heel pain in many ways, including. Wear shoes that fit you properly with a firm fastening, such as laces. Choose shoes with shock-absorbent soles and supportive heels. Repair or throw out any shoes that have worn heels. Always warm up and cool down when exercising or playing sport, include plenty of slow, sustained stretches. If necessary, your podiatrist will show you how to tape or strap your feet to help support the muscles and ligaments. Shoe inserts (orthoses) professionally fitted by your podiatrist can help support your feet in the long term.
Leg Length Discrepancy Test
Overview
leg length discrepancy can be present from birth (congenital) or acquired (a result of an injury, infection or tumor). Some of the conditions that can cause limb problems in a child or young adult include congenital conditions present from birth. Osteogenesis imperfecta,. Bow legs. Knock knees. Neurofibromatosis. Arthritis. Infections of the bones and tumors. Injuries involving the growth center of the bone. There may also be deformities that are a result of the soft tissues and not the bones, such as with arthrogryposis and burns.
Causes
The causes of LLD are many, including a previous injury, bone infection, bone diseases (dysplasias), inflammation (arthritis) and neurologic conditions. Previously broken bones may cause LLD by healing in a shortened position, especially if the bone was broken in many pieces (comminuted) or if skin and muscle tissue around the bone were severely injured and exposed (open fracture). Broken bones in children sometimes grow faster for several years after healing, causing the injured bone to become longer. Also, a break in a child?s bone through a growth center (located near the ends of the bone) may cause slower growth, resulting in a shorter extremity. Bone infections that occur in children while they are growing may cause a significant LLD, especially during infancy. Bone diseases may cause LLD, as well; examples are neurofibromatosis, multiple hereditary exostoses and Ollier disease. Inflammation of joints during growth may cause unequal extremity length. One example is juvenile rheumatoid arthritis. Osteoarthritis, the joint degeneration that occurs in adults, very rarely causes a significant LLD.
Symptoms
Patients with significant lower limb length discrepancies may walk with a limp, have the appearance of a curved spine (non-structural scoliosis), and experience back pain or fatigue. In addition, clothes may not fit right.
Diagnosis
The evaluation of leg length discrepancy typically involves sequential x-rays to measure the exact discrepancy, while following its progression. In addition, an x-ray of the wrist allows us to more carefully age your child. Skeletal age and chronological age do not necessarily equal each other and frequently a child's bone age will be significantly different than his or her stated age. Your child's physician can establish a treatment plan once all the facts are known: the bone age, the exact amount of discrepancy, and the cause, if it can be identified.
Non Surgical Treatment
Treatment is based on an estimate of how great the difference in leg length will be when the child grows up, Small differences (a half inch or less) do not need treatment. Differences of a half to one inch may require a lift inside the shoe.

how to grow taller at 14
Surgical Treatment
In growing children, legs can be made equal or nearly equal in length with a relatively simple surgical procedure. This procedure slows down the growth of the longer leg at one or two growth sites. Your physician can tell you how much equalization can be gained by this procedure. The procedure is performed under X-ray control through very small incisions in the knee area. This procedure will not cause an immediate correction in length. Instead, the limb length discrepancy will gradually decrease as the opposite extremity continues to grow and "catch up." Timing of the procedure is critical. The goal is to reach equal leg length by the time growth normally ends. This is usually in the mid-to-late teenage years. Disadvantages of this option include the possibility of slight over-correction or under-correction of the limb length discrepancy. In addition, the patient's adult height will be less than if the shorter leg had been lengthened. Correction of significant limb length discrepancy by this method may make a patient's body look slightly disproportionate because of the shorter leg. In some cases the longer leg can be shortened, but a major shortening may weaken the muscles of the leg. In the thighbone (femur), a maximum of 3 inches can be shortened. In the shinbone, a maximum of 2 inches can be shortened.
leg length discrepancy can be present from birth (congenital) or acquired (a result of an injury, infection or tumor). Some of the conditions that can cause limb problems in a child or young adult include congenital conditions present from birth. Osteogenesis imperfecta,. Bow legs. Knock knees. Neurofibromatosis. Arthritis. Infections of the bones and tumors. Injuries involving the growth center of the bone. There may also be deformities that are a result of the soft tissues and not the bones, such as with arthrogryposis and burns.
Causes
The causes of LLD are many, including a previous injury, bone infection, bone diseases (dysplasias), inflammation (arthritis) and neurologic conditions. Previously broken bones may cause LLD by healing in a shortened position, especially if the bone was broken in many pieces (comminuted) or if skin and muscle tissue around the bone were severely injured and exposed (open fracture). Broken bones in children sometimes grow faster for several years after healing, causing the injured bone to become longer. Also, a break in a child?s bone through a growth center (located near the ends of the bone) may cause slower growth, resulting in a shorter extremity. Bone infections that occur in children while they are growing may cause a significant LLD, especially during infancy. Bone diseases may cause LLD, as well; examples are neurofibromatosis, multiple hereditary exostoses and Ollier disease. Inflammation of joints during growth may cause unequal extremity length. One example is juvenile rheumatoid arthritis. Osteoarthritis, the joint degeneration that occurs in adults, very rarely causes a significant LLD.
Symptoms
Patients with significant lower limb length discrepancies may walk with a limp, have the appearance of a curved spine (non-structural scoliosis), and experience back pain or fatigue. In addition, clothes may not fit right.
Diagnosis
The evaluation of leg length discrepancy typically involves sequential x-rays to measure the exact discrepancy, while following its progression. In addition, an x-ray of the wrist allows us to more carefully age your child. Skeletal age and chronological age do not necessarily equal each other and frequently a child's bone age will be significantly different than his or her stated age. Your child's physician can establish a treatment plan once all the facts are known: the bone age, the exact amount of discrepancy, and the cause, if it can be identified.
Non Surgical Treatment
Treatment is based on an estimate of how great the difference in leg length will be when the child grows up, Small differences (a half inch or less) do not need treatment. Differences of a half to one inch may require a lift inside the shoe.
how to grow taller at 14
Surgical Treatment
In growing children, legs can be made equal or nearly equal in length with a relatively simple surgical procedure. This procedure slows down the growth of the longer leg at one or two growth sites. Your physician can tell you how much equalization can be gained by this procedure. The procedure is performed under X-ray control through very small incisions in the knee area. This procedure will not cause an immediate correction in length. Instead, the limb length discrepancy will gradually decrease as the opposite extremity continues to grow and "catch up." Timing of the procedure is critical. The goal is to reach equal leg length by the time growth normally ends. This is usually in the mid-to-late teenage years. Disadvantages of this option include the possibility of slight over-correction or under-correction of the limb length discrepancy. In addition, the patient's adult height will be less than if the shorter leg had been lengthened. Correction of significant limb length discrepancy by this method may make a patient's body look slightly disproportionate because of the shorter leg. In some cases the longer leg can be shortened, but a major shortening may weaken the muscles of the leg. In the thighbone (femur), a maximum of 3 inches can be shortened. In the shinbone, a maximum of 2 inches can be shortened.
Mortons Neuroma Solutions
Overview
 Some sources claim that entrapment of the plantar nerve because of compression between the metatarsal heads, as originally proposed by Morton, is highly unlikely, because the plantar nerve is on the plantar side of the transverse metatarsal ligament and thus does not come in contact with the metatarsal heads. It is more likely that the transverse metatarsal ligament is the cause of the entrapment. Despite the name, the condition was first correctly described by a chiropodist named Durlacher, and although it is labeled a "neuroma", many sources do not consider it a true tumor, but rather a perineural fibroma (fibrous tissue formation around nerve tissue).
Some sources claim that entrapment of the plantar nerve because of compression between the metatarsal heads, as originally proposed by Morton, is highly unlikely, because the plantar nerve is on the plantar side of the transverse metatarsal ligament and thus does not come in contact with the metatarsal heads. It is more likely that the transverse metatarsal ligament is the cause of the entrapment. Despite the name, the condition was first correctly described by a chiropodist named Durlacher, and although it is labeled a "neuroma", many sources do not consider it a true tumor, but rather a perineural fibroma (fibrous tissue formation around nerve tissue).
Causes
The exact cause is as yet unclear. However there are a number of theories. Some expert s believe problems with the design of the foot makes some people more prone to Morton?s neuroma. Having flat feet or a high arch for example encourages the foot to slide forwards which can put excess pressure on the metatarsals. Bunions and hammer toes also increase the likelihood of developing Morton?s. However simply wearing high heels or any form of tight shoes that put pressure on the bones in the feet can also lead to a Morton?s . Typically the condition comes on between the age of 40 and 50. It is far more common in women than men - three out of four sufferers are women.
Symptoms
The most common symptom of Morton's neuroma is localized pain in the interspace between the third and fourth toes. It can be sharp or dull, and is worsened by wearing shoes and by walking. Pain usually is less severe when the foot is not bearing weight.
Diagnosis
In some cases your doctor will be able to feel the Morton's as a swelling in the middle of your foot. However they may also suggest an X-ray or a blood test - this is normally to rule our other causes of the pain such as arthritis. The most accurate way to diagnose Morton?s itself is with magnetic resonance imaging (MRI) or ultrasound.
Non Surgical Treatment
Ice therapy and anti-inflammatory medications or supplements. If conservative care measures fail to resolve your problem, some foot care providers may recommend a cortisone injection around your involved nerve to help reduce your swelling and inflammation. Concentrated alcohol injections around your affected nerve have also shown good results and should be considered before undergoing neurectomy, a surgical procedure to remove the enlarged, traumatized portion of your involved nerve.
Surgical Treatment
If pain persists with conservative care, surgery may be an appropriate option. The common digitial nerve is cut and the Mortons neuroma removed. This will result is numbness along the inside of the toes affected, and there is a small chance the end of the nerve will form a Stump Neuroma. Approximately 75% of people receive symptom resolution for Mortons Neuroma with conservative care.
Some sources claim that entrapment of the plantar nerve because of compression between the metatarsal heads, as originally proposed by Morton, is highly unlikely, because the plantar nerve is on the plantar side of the transverse metatarsal ligament and thus does not come in contact with the metatarsal heads. It is more likely that the transverse metatarsal ligament is the cause of the entrapment. Despite the name, the condition was first correctly described by a chiropodist named Durlacher, and although it is labeled a "neuroma", many sources do not consider it a true tumor, but rather a perineural fibroma (fibrous tissue formation around nerve tissue).Causes
The exact cause is as yet unclear. However there are a number of theories. Some expert s believe problems with the design of the foot makes some people more prone to Morton?s neuroma. Having flat feet or a high arch for example encourages the foot to slide forwards which can put excess pressure on the metatarsals. Bunions and hammer toes also increase the likelihood of developing Morton?s. However simply wearing high heels or any form of tight shoes that put pressure on the bones in the feet can also lead to a Morton?s . Typically the condition comes on between the age of 40 and 50. It is far more common in women than men - three out of four sufferers are women.
Symptoms
The most common symptom of Morton's neuroma is localized pain in the interspace between the third and fourth toes. It can be sharp or dull, and is worsened by wearing shoes and by walking. Pain usually is less severe when the foot is not bearing weight.
Diagnosis
In some cases your doctor will be able to feel the Morton's as a swelling in the middle of your foot. However they may also suggest an X-ray or a blood test - this is normally to rule our other causes of the pain such as arthritis. The most accurate way to diagnose Morton?s itself is with magnetic resonance imaging (MRI) or ultrasound.
Non Surgical Treatment
Ice therapy and anti-inflammatory medications or supplements. If conservative care measures fail to resolve your problem, some foot care providers may recommend a cortisone injection around your involved nerve to help reduce your swelling and inflammation. Concentrated alcohol injections around your affected nerve have also shown good results and should be considered before undergoing neurectomy, a surgical procedure to remove the enlarged, traumatized portion of your involved nerve.
Surgical Treatment
If pain persists with conservative care, surgery may be an appropriate option. The common digitial nerve is cut and the Mortons neuroma removed. This will result is numbness along the inside of the toes affected, and there is a small chance the end of the nerve will form a Stump Neuroma. Approximately 75% of people receive symptom resolution for Mortons Neuroma with conservative care.
Shoe Lifts For Leg Length Discrepancy
There are not one but two different kinds of leg length discrepancies, congenital and acquired. Congenital implies you are born with it. One leg is structurally shorter compared to the other. As a result of developmental periods of aging, the human brain picks up on the step pattern and recognizes some variation. The human body usually adapts by tilting one shoulder over to the "short" side. A difference of less than a quarter inch isn't blatantly uncommon, does not need Shoe Lifts to compensate and in most cases won't have a profound effect over a lifetime.

Leg length inequality goes largely undiscovered on a daily basis, yet this problem is very easily corrected, and can eradicate a number of cases of upper back pain.
Treatment for leg length inequality commonly involves Shoe Lifts. These are generally very reasonably priced, in most cases priced at less than twenty dollars, in comparison to a custom orthotic of $200 or more. Differences over a quarter inch can take their toll on the spine and should probably be compensated for with a heel lift. In some cases, the shortage can be so extreme that it requires a full lift to both the heel and sole of the shoe.
Upper back pain is easily the most prevalent health problem impacting people today. Over 80 million people have problems with back pain at some stage in their life. It's a problem that costs companies millions annually due to time lost and productivity. New and better treatment methods are always sought after in the hope of decreasing the economical impact this issue causes.

Men and women from all corners of the world suffer from foot ache as a result of leg length discrepancy. In most of these cases Shoe Lifts might be of worthwhile. The lifts are capable of alleviating any pain in the feet. Shoe Lifts are recommended by countless specialist orthopaedic physicians.
So as to support the human body in a well-balanced manner, feet have got a significant task to play. Irrespective of that, it's often the most neglected zone of the human body. Many people have flat-feet which means there may be unequal force placed on the feet. This will cause other areas of the body like knees, ankles and backs to be affected too. Shoe Lifts make sure that suitable posture and balance are restored.
Leg length inequality goes largely undiscovered on a daily basis, yet this problem is very easily corrected, and can eradicate a number of cases of upper back pain.
Treatment for leg length inequality commonly involves Shoe Lifts. These are generally very reasonably priced, in most cases priced at less than twenty dollars, in comparison to a custom orthotic of $200 or more. Differences over a quarter inch can take their toll on the spine and should probably be compensated for with a heel lift. In some cases, the shortage can be so extreme that it requires a full lift to both the heel and sole of the shoe.
Upper back pain is easily the most prevalent health problem impacting people today. Over 80 million people have problems with back pain at some stage in their life. It's a problem that costs companies millions annually due to time lost and productivity. New and better treatment methods are always sought after in the hope of decreasing the economical impact this issue causes.
Men and women from all corners of the world suffer from foot ache as a result of leg length discrepancy. In most of these cases Shoe Lifts might be of worthwhile. The lifts are capable of alleviating any pain in the feet. Shoe Lifts are recommended by countless specialist orthopaedic physicians.
So as to support the human body in a well-balanced manner, feet have got a significant task to play. Irrespective of that, it's often the most neglected zone of the human body. Many people have flat-feet which means there may be unequal force placed on the feet. This will cause other areas of the body like knees, ankles and backs to be affected too. Shoe Lifts make sure that suitable posture and balance are restored.
The Best Ways To Protect Against Posterior Calcaneal Spur

Overview
Although a heel spur is often thought to be the source of heel pain, it rarely is. When a patient has plantar fasciitis, the plantar fascia pulls on the bottom of the heel bone. Over time this can cause a spur to form. Heels spurs are a very common x-ray finding, and because the heel spur is buried deep in soft tissue and not truly in a weight bearing area, there is often no history of pain. It is important to note that less than one percent of all heel pain is due to a spur. but frequently caused by the plantar fascia pulling on the heel. Once the plantar fasciitis is properly treated, the heel spur could be a distant memory.
Causes
There exists a membrane that covers most of the bone along the heel. When this membrane gets torn repeatedly due to straining of the muscles in the foot, the calcium deposits that lead to heel spurs are more likely to occur.

Symptoms
Heel spurs result in a jabbing or aching sensation on or under the heel bone. The pain is often worst when you first arise in the morning and get to your feet. You may also experience pain when standing up after prolonged periods of sitting, such as work sessions at a desk or car rides. The discomfort may lessen after you spend several minutes walking, only to return later. Heel spurs can cause intermittent or chronic pain.
Diagnosis
A Heel Spur diagnosis is made when an X-ray shows a hook of bone protruding from the bottom of the foot at the point where the plantar fascia is attached to the heel bone. The plantar fascia is the thick, connective tissue that runs from the calcaneus (heel bone) to the ball of the foot. This strong and tight tissue helps maintain the arch of the foot. It is also one of the major transmitters of weight across the foot as you walk or run. In other words, tremendous stress is placed on the plantar fascia.
Non Surgical Treatment
If pain and other symptoms of inflammation-redness, swelling, heat-persist, you should limit normal daily activities and contact a doctor of podiatric medicine. The podiatric physician will examine the area and may perform diagnostic X-rays to rule out problems of the bone. Early treatment might involve oral or injectable anti-inflammatory medication, exercise and shoe recommendations, taping or strapping, or use of shoe inserts or orthotic devices. Taping or strapping supports the foot, placing stressed muscles and tendons in a physiologically restful state. Physical therapy may be used in conjunction with such treatments. A functional orthotic device may be prescribed for correcting biomechanical imbalance, controlling excessive pronation, and supporting of the ligaments and tendons attaching to the heel bone. It will effectively treat the majority of heel and arch pain without the need for surgery. Only a relatively few cases of heel pain require more advanced treatments or surgery. If surgery is necessary, it may involve the release of the plantar fascia, removal of a spur, removal of a bursa, or removal of a neuroma or other soft-tissue growth.
Surgical Treatment
Though conservative treatments for heel spurs work most of the time, there are some cases where we need to take your treatment to the next level. Luckily, with today?s technologies, you can still often avoid surgery. Some of the advanced technologies to treat a Heel Spur are Platelet Rich Plasma Therapy. Platelet Rich Plasma Therapy (also known as PRP) is one of several regenerative medicine techniques that University Foot and Ankle Institute has helped bring to foot and ankle care. This amazing in-office procedure allows the growth factors in the blood to be used to actually begin the healing process again long after your body has given up on healing the area. Heel Pain Shockwave Therapy. Shockwave therapy is a non-invasive procedure done in the office that allows for new blood to get to the region of fascia damage and help with healing. Results have been excellent with more than 70 percent of patients getting relief with only one treatment. Topaz for Heal Spurs and pain. Another minimally invasive technology technique is called Coblation Surgery using a Topaz probe. This minimally invasive procedure involves controlled heating of multiple tiny needles that are inserted through the skin and into the plantar fascia. This process, like PRP and Shockwave therapy, irritates the fascia enough to turn a chronic problem back into an acute problem, greatly increasing the chances of healing. Heel Spur Surgery. Endoscopic Plantar Fasciotomy is one surgical procedure that we consider to release the tight fascia. University Foot and Ankle Institute has perfected an endoscopic (camera guided) approach for fascia release to allow rapid healing and limited downtime with minimal pain.
Prevention
In 2002, researchers attempted to compare the effects of various running techniques on pronation and resulting injuries like stress fractures and heel spurs. They suggested that it is possible to teach runners to stride in such a way as to minimize impact forces. One way is to lower running speed. Another is to take longer rest periods following a run.